
MIPS guide in 10 steps
A practical guide to help provider organizations understand the factors impacting MIPS score and how to improve it.
MIPS is not just a reporting requirement. It is a year-long coordination effort across product, compliance, operations, clinical leadership, and reporting teams. The challenge is not simply understanding the rules. It is knowing what needs to happen, when it needs to happen, and which teams need to be aligned at each stage.
This guide breaks the journey into 3 phases and 10 steps so teams can move through MIPS in a structured way, hand off work clearly, and focus on the decisions that matter most.
It includes guidance to help organizations determine the key determinants for each step and identify the areas where they need support from MIPS experts:
EHRs - managing regulatory readiness, certified capabilities, measure support, validation, and submission workflows
Provider organizations - managing performance, documentation, operational execution, and successful reporting
🔶MIPS performance in 2026 affects the 2028 Medicare Part B payment adjustment. This makes early decisions more valuable than late cleanup.🔶MIPS at a glance
Quality
Weight: 30%
Reporting: Full year
Focus: Performance and data capture
Cost
Weight: 30%
Reporting: Full year
Focus: Claims-based performance. No submission
Promoting Interoperability
Weight: 25%
Reporting: 180 days
Focus: Performance and attestation
Improvement Activities
Weight: 15%
Reporting: 90 days
Focus: Completion and documentation
Phase 1 - Set the Reporting Foundation
This phase sets the direction for the rest of the year. It defines the reporting path, the level of responsibility, and the measure and workflow requirements that downstream teams will have to support.
If the reporting foundation is not set clearly on time, all subsequent MIPS-related efforts become harder to coordinate and more expensive to fix.
Step 1. Confirm your MIPS reporting strategy
Your reporting path shapes everything that follows, from measure selection and workflow requirements to scoring logic and submission readiness. That means choosing the reporting pathway that fits best - Traditional MIPS, MIPS Value Pathways (MVPs), or Advanced Alternative Payment Models (Advanced APMs), and then deciding whether reporting will happen at the individual or group level.
The challenge
Many organizations treat reporting strategy as a basic administrative choice. It is not. It affects reporting flexibility, ownership, aggregation, scoring, and submission.
Why this decision matters
When the reporting path isn't locked in early, teams start building on the wrong assumptions. EHRs may not support the chosen path's logic or data structure, or may not have the required ONC certification. Provider organizations may underestimate the coordination needed for group reporting across specialties or locations.
For EHRs

- Confirm which MIPS reporting pathways and measures (Quality and PI) will be supported
- Align measure logic, aggregation, validation, and output expectations accordingly
- Understand how the chosen path affects implementation and support burden
For Provider Orgs
- Decide whether performance risk sits with individual providers or the group
- Align the reporting strategy with specialty mix, operational structure, and regulatory requirements
- Assign a clear MIPS owner early
What to review now →
Individual vs Group reporting
Traditional MIPS vs MVP vs MIPS APM
Facility-based and special-status (small practice, non-patient-facing, etc) implications
Clear ownership of MIPS responsibilities across the organization
Reporting Level: Individual vs Group Reporting
| Reporting level | How performance is scored | What EHRs need to support | What Provider Orgs need to weigh |
|---|---|---|---|
| Individual | Score is calculated per NPI | Clinician-level tracking, validation, and output readiness | Performance risk stays with each clinician and may be easier to isolate |
| Group | Single score across the TIN | TIN-level aggregation, denominator alignment, consistent capture across sites, and cleaner cross-site validation | Performance and resulting payment adjustment are shared across the organization (including MIPS ineligible NPIs) and require tighter operational coordination |
Reporting Pathway Options: Traditional MIPS vs MVP vs MIPS APM
| Pathway | Best fit for | The Benefits | Main trade-off |
|---|---|---|---|
| Traditional MIPS | Organizations that need broader measure flexibility | More choice in measure selection and more room to optimize | More measure-selection work and decision complexity |
| MVP | Organizations that want a more specialty-aligned path | Fewer measures and activities to report are predefined, with less room to improvise later | Less flexibility once selected |
| MIPS APM | Organizations already operating within an applicable APM structure | Scoring and reporting responsibilities shift based on the APM model | Different reporting logic and governance requirements |
Where MyMipsScore adds value
MyMipsScore helps EHRs and enterprise provider organizations evaluate reporting pathways based on feasibility and scoring potential, understand support implications, and align the reporting model with certification, validation, and submission requirements.
Review your MIPS reporting and support strategy→
Step 2. Understand what changes with MVP Reporting
If the MIPS Value Pathway (MVP) is under consideration, this is the point at which teams need to evaluate the interplay of the reduced reporting burden with scoring and reporting readiness. MVPs include a foundational layer that is the same for all the MVPs. This layer includes two population health measures (calculated by CMS) and all the PI measures applicable for the Traditional MIPS.
The challenge
MVPs reduce the reporting burden (4 Quality measures vs 6; only one IA for all practice sizes). Most MVPs include a mix of EHR (eCQMs) and Registry measures (MIPS CQMs). Some MVPs include Quality measures and Improvement Activities that are only available within that MVP. That could require changes to the usual MIPS measure (tracking and supporting) workflows that an EHR or provider organization is used to.
That also means less flexibility later if workflows, data capture, PI support, IA execution, or Quality performance do not line up. It is not just a reporting choice. It is a different operating model - one worth considering with 6 new MVPs and all 21 existing MVPs modified.
What MVP reporting shapes downstream
MVPs reduce the reporting burden (4 Quality measures vs 6; only one IA for all practice sizes). That also means less flexibility later if workflows, data capture, PI support, IA execution, or Quality performance do not line up. It is not just a reporting choice. It is a different operating model – one worth considering with 6 new MVPs and all 21 existing MVPs modified.
For EHRs
- Confirm support for MVP-aligned Quality measures (eCQMs and MIPS CQMs) and submission pathways
- Verify structured capture of required data elements
- Ensure PI and IA support is evaluated in the context of MVP requirements, not in isolation
- Confirm registry-based submission workflows support MVP reporting
For Provider Orgs
- Confirm the MVP aligns with specialty, care delivery, and documentation habits
- Understand registration requirements and deadlines — Registration opened on April 1, 2026
- Assess whether the organization can support the required workflows consistently across locations and teams
- Confirm that the included Quality measures are realistic in practice
What to review now →
Relevant MVP options by specialty to support (for EHRs) or to report (for providers) (6 new and 21 existing modified)
Included Quality measures and their scoring potential, and Improvement Activities
Whether the EHR and reporting solution support all Quality measures in the selected MVP(s)
Whether workflows can support the required data capture
How MyMipsScore supports MVP readiness
MyMipsScore helps teams assess MVP readiness before committing to a specific MVP, covering Quality, PI, IA, workflow feasibility, scoring implications, and submission alignment.
Assess your MVP readiness →
Tip
Do not evaluate an MVP simply as a shorter list of measures. Evaluate whether the EHR can support and whether the provider organization can score well on those measures.
Step 3. Define what you need to report
Once the reporting strategy is clear, define the reporting scope, including all applicable measures, activities, attestations, MIPS Qualified Registry integrations, and supporting workflows.
The challenge
Teams often choose what looks clinically relevant or familiar without fully testing whether it is current, supported by EHR, scores well, or is realistic in actual workflow.
Where risk builds
A measure may be clinically relevant yet still perform poorly under MIPS scoring. By the time teams realize a measure is topped out, has a high benchmark, is unsupported, or hard to capture reliably, a few months have gone by, and the scoring opportunity has already been lost.
For EHRs
- Confirm only current-year measures appear in the system
- Remove outdated measures and update logic for 2026 measures
- Verify structured data capture and calculation support for each measure
- Ensure supported measures align with both Traditional MIPS and relevant MVP paths
- Confirm PI and IA support tied to the selected MIPS reporting path
For Provider Organizations
- Shortlist measures based on care delivery, data capture reliability, and scoring potential
- Avoid defaulting to familiar measures or past reporting approaches
- Ensure selected measures work across providers, specialties, and locations
- Evaluate Quality measure case volume and benchmark changes early
- Measures available as eCQMs generally score better than their MIPS CQM versions
What to review now →
Six Quality measures under Traditional MIPS, unless the specialty set has fewer
Outcome or High Priority measure requirement if no Outcome measure applies
Current-year benchmarks, topped-out status, and case-volume feasibility
Any changes to the supported or previously reported Improvement Activities
PI attestation and ONC certification dependencies
What makes a measure worth keeping
| What to confirm | |
|---|---|
| Current | Is it valid for the 2026 performance year? |
| Supported | Is the logic implemented correctly in the EHR and MIPS Registry? |
| Feasible | Can providers reliably capture the required data in their workflow? |
| Scorable | Is it topped out, has a high benchmark, or likely to miss the case minimum (20 patients)? |
How MyMipsScore helps teams move forward
MyMipsScore helps align reporting scope with current CMS logic, measure updates (versions and calculations), benchmark realities, and workflow feasibility so teams are not building around measures that look good on paper but fail in execution.
Review your 2026 MIPS measures selection →
Phase 2 - Execute Across the Performance Categories
This phase is where strategy becomes operational. Different teams may own different pieces of the MIPS strategy, which is exactly why a clear understanding of the requirements for Quality, PI, IA, and Cost is essential for effective execution and clean handoff.
Step 4. Lock in Improvement Activities early
Of all the performance categories, Improvement Activities (IA) look the most manageable, which is exactly why they often get pushed down the priority list.
The challenge
IA is usually not where organizations lose points because the rules are too complex. They lose points due to unclear ownership, insufficient attention to activity selection, or inadequate documentation.
What has to work together
Activity choice, participation, documentation, and audit support all need to line up. In MVP, that gets more important because included activities may be more constrained and less forgiving of loose execution.
For EHRs
- Help customers understand what IA support looks like in practice
- Clarify documentation expectations and audit considerations
- For MVP, make sure the required support for included activities is understood early
For Provider Orgs
- Choose activities that align with everyday work
- Confirm participation thresholds
- Make documentation easy to produce and verifiable
- For MVP, confirm the included activities are realistic across intended providers and locations
What to review now →
Minimum 90 consecutive-days requirement
Special-status eligibility
Patient-Centered Medical Home full-credit implications
Group participation threshold of at least 50% of providers in the TIN
MVP-included activities where applicable
IA requirement by reporting status
Individual with special status
Attest to 1 activity for full credit
Group with 15 or fewer providers
Attest to 1 activity for full credit
Group with more than 15 providers
Attest to 2 activities for full credit
Any entity reporting a MVP
Attest to 1 activity for full credit
Where MyMipsScore helps
MyMipsScore helps teams plan for IA earlier, align activity selection with the reporting path, and keep documentation expectations visible before attestation and submission time.
Validate your IA planning →
Tip
If an Improvement Activity depends on cross-site participation, name the owner, documentation process, and evidence source early.
Step 5. Determine Promoting Interoperability (PI) applicability and readiness
The Promoting Interoperability (PI) category evaluates how providers use a certified EHR to exchange information, prescribe electronically, and provide patients with access to their health records. So, EHRs supporting MIPS-eligible providers need to support and be certified for all the underlying ONC criteria by default.
Before provider organizations prepare for reporting PI, they need to know whether it applies, whether it will be reweighted, or whether a hardship exception must be considered.
The Challenge
EHRs often fail to account for MIPS applicability to certain ONC certification criteria, such as FHIR APIs required for information exchange between providers and patients, and to prevent Information Blocking. Provider organizations often fail to clearly distinguish between PI applicability and PI execution. These are not the same, different decisions, which could be further complicated for multi-location and multi-specialty setups
Why does this need to be addressed early
For EHRs, certifying or integrating with an ONC-certified modular health IT solution will take time if they don’t already have it. For providers, a late PI applicability evaluation can distort the entire scoring plan. If PI is reweighted, it will change category weighting and can increase pressure on Quality and other categories.
For EHRs
- Make PI-related MIPS reporting support explicit
- Confirm ONC certification required to support PI measures, including (g)(10) FHIR API
- Assess PI support across both Traditional MIPS and MVP requirements
For Provider Organizations
- Confirm whether PI applies to the group or selected providers
- Evaluate hardship or reweighting eligibility early
- Understand how PI reweighting affects the broader scoring strategy
What to review now →
Is your EHR certified for supporting all PI measures
Data capture for all the PI measure calculations and attestations
Automatic reweighting eligibility
Hardship exception eligibility
Clinician types no longer automatically reweighted
PI applicability decision guide
| Question | If yes | If no |
|---|---|---|
| Does the clinician or group qualify for automatic reweighting? | PI weight moves to another category under CMS rules | Move to hardship review |
| Is a hardship exception justified and approved? | PI is reweighted per CMS rules | PI must be reported |
| Does the current EHR support the required PI measures? | Proceed with PI readiness planning | Resolve the support gap early |
How MyMipsScore supports this step
MyMipsScore helps EHRs quickly assess and address the PI readiness gap and applicability. Provider organizations will gain clarity on the PI category reweighting implications, identify support gaps, and select the optimal performance period (minimum 180 days).
Review your PI readiness or eligibility →
Step 6. Keep Promoting Interoperability (PI) workflows on track
This is the step that demands close alignment between the EHR's capabilities and how providers use them. If PI is reportable, the focus of the provider organizations shifts to uniform data capture and tracking across their multiple locations and groups for the reporting period.
The challenge
Many teams assume that having certified technology is enough. It is not. PI performance depends on workflow use, documentation, and consistent data capture for reporting over time.
What teams need to be aligned
The PI workflows need to be used consistently across providers and locations for the reporting period. PI is part of the MVP foundational layer and is applicable unless the provider reporting entity qualifies for reweighting.
For EHRs
- Ensure PI functionality is usable, reliable, and correctly implemented
- Check that attestations and reporting outputs align with MIPS requirements
- Explicitly show customers how PI measures are supported within the EHR
For Provider Organizations
- Choose and protect the 180-day minimum reporting period
- Maintain consistent workflows across providers and locations
- Complete SRA, SRM, SAFER Guides review, and required documentation
What to review now →
Optimum consecutive 180-day minimum reporting period
Security Risk Analysis (SRA) 🛑
Security Risk Management (SRM) ⚡🛑
SAFER Guides review 🛑
Core workflows such as e-prescribing, patient access, exchange of summaries, and public health reporting
⚡New requirement added in 2026🛑 Must have a positive attestation to earn a score in PI
Where MyMipsScore supports execution
MyMipsScore helps teams keep PI workflows aligned with MIPS certification and reporting requirements. We help teams identify and reduce the risk of failure caused by inconsistent or missing documentation or data capture.
Review your PI workflow readiness →
Tip
For the Provider-to-Patient exchange PI measure, all patients must have access to a patient portal and use a third-party app of their choice to access their health information to earn credit and earn a score for the PI category. No exemptions.
Step 7. Understand Cost exposure
Cost is part of the final MIPS score, but it is different from the other categories. Providers do not submit Cost data directly, and EHRs have no direct role in Cost calculation. That is exactly why it needs to be properly placed within the overall MIPS strategy.
The challenge
Teams either overlook Cost because it isn’t reportable and calculated by CMS from administrative claims or assume it doesn’t apply to them in 2026 because it didn’t in the previous year(s). New measures are added each year, and attributable episodes vary.
What is at stake
Cost carries the same weight as Quality, cannot be submitted directly, and cannot be cleaned up at the end. If leadership is ignorant of the impact of this category on the MIPS score or has unrealistic expectations for performance in this category, the overall MIPS strategy becomes unbalanced.
For EHRs
- Help customers understand utilization and coding patterns that impact Cost
- Support Cost measure tracking and visibility where possible
For Provider Organizations
- Review prior Cost feedback if available
- Understand attributable episodes and triggered measures
- Set realistic expectations by specialty, location, and care delivery
What to review now →
Prior-year Cost feedback in the QPP portal, if available
Triggered or newly attributable Cost measures
Attributable episodes
Minimum case-volume implications
What you can and cannot do for the Cost category
| You can | You cannot |
|---|---|
| Review prior utilization patterns | Select measures and submit data for them |
| See which measures were triggered | Fix the category through extra effort at the end of the year |
| Determine likely future exposure | Rely on the EHR alone to track likely applicable measures |
How MyMipsScore supports Cost
MyMipsScore helps organizations place Cost in the right strategic context, so it informs planning without creating false confidence about what can be repaired later.
Review your Cost exposure →
Step 8. Choose and validate Quality measures
Quality is too important to treat as a one-time selection exercise. The right measures need to be chosen, monitored, supported, and validated based on how CMS will score them.
The challenge
Teams often choose measures because they align loosely with a specialty or are easy to support and report. Upon proper review in the context of data capture for the measure and current benchmark, they discover that it’s difficult to reliably capture the data for those measures, and they are unlikely to score well because of their topped-out status or high benchmark.
Where ignorance gets expensive
Quality carries a significant scoring weight (30%) for MIPS, and even more if PI is reweighted. If teams choose the wrong measures, don’t have access to a dashboard for year-round tracking, or rely on outdated dashboards or CMS scoring logic, a full year of effort can yield disappointing results. For an MVP, accuracy and precision are even more important because there are only 4 Quality measures to report from a much smaller pool.
For EHRs
- Support 2026 measures, versions, and logic for eCQMs and MIPS CQMs
- Confirm structured data capture for all current and supported measures
- Validate data formats for transmission to registries and CMS
- Ensure supported measures align with both Traditional MIPS and specialty-relevant MVPs
For Provider Organizations
- Select measures based on care delivery and scoring potential
- Consider workflow reliability across locations and specialties
- Monitor more measures than the minimum required to report, where feasible
- For MVP, confirm that included Quality measures are supported and likely to score well
What to review now →
Availability of the measures reported for 2025 or earlier
Topped-out status of these measures
One measure must be an ‘Outcome’ measure (or ‘High Priority’ measure if an Outcome measure isn’t available)
Benchmark changes and differences between eCQMs and MIPS CQMs
Data capture and workflow consistency across providers and locations
Availability of the dashboard for year-round performance tracking, with the 2026 measures and scoring logic
Quality measure check
| Criteria | What to confirm |
|---|---|
| Clinically relevant | Fits the actual scope of care |
| Technically supported | Logic and required data elements are available |
| Scorable | Benchmark and topped-out status are acceptable |
| Sufficient volume | Likely to meet the case minimum |
| Operationally reliable | Data can be captured consistently across providers and locations |
What to validate before Quality measure submission
Measure benchmark
Each measure can earn up to 10 points (7 points for topped-out measures).
- More than 15 providers: measures without a benchmark score 0 points
- 15 or fewer providers: see Small Practice
Data completeness
At least 75% of eligible patients must be reported.
- More than 15 providers: below 75% scores 0 points
- 15 or fewer providers: see Small Practice
Case minimum
A measure must have at least 20 cases.
- More than 15 providers: below 20 cases score 0 points
- 15 or fewer providers: see Small Practice
Small Practice
Practices with 15 or fewer providers receive the following flexibilities:
- 3 points if a measure has no benchmark
- 3 points if data completeness is not met
- 3 points if case minimum is not met
- 6 bonus points in Quality if at least one measure is submitted
How MyMipsScore helps improve Quality category performance
MyMipsScore helps EHRs support all 2026 Quality measures, including eCQMs and MIPS CQMs, through its ONC-Certified module and CMS Qualified Registry. This helps EHRs provide integrated MIPS support to their users.
Provider organizations using MyMipsScore, either directly or through an integrated EHR, get year-round access to an easy-to-use MIPS dashboard. The dashboard helps them track measures, compare scoring potential, and choose the measures that are most likely to perform well based on their results, available benchmarks, and MIPS scoring rules. This enables providers to execute a Quality reporting strategy based on the measures that work best for their practice.
Validate your Quality performance readiness →
Tips
A Quality measure available for reporting is not automatically a strong reporting choice.
eCQMs generally score better than MIPS-CQMs for the same performance.
Monitor more Quality measures than required to report to maximize your Quality score.
Step 9. Prepare for final submission
Submission should be treated as the final validation checkpoint, not as the initial test of the entire IA, PI, and Quality performance capture, aggregation, and submission process.
The Challenge
Teams often treat submissions as a handoff or file-transfer step. In reality, this is where hidden gaps become visible (and panic strikes).
What gets amplified at this step
Missing or non-functional ONC certification (FHIR APIs fulfill patients’ requests for information), outdated or incorrect measure logic, unsupported formats, incomplete attestations (PI), and missing documentation (for IA) tend to surface at this point. If teams are attempting to work together and align for the first time at submission, the risk is already very high.
For EHRs
- Validate measure logic end-to-end - from capture, data format for export, to submission
- Confirm compliance with the required ONC certifications to support MIPS (Quality and PI)
- Test and validate that data aggregation and export workflows are working
- Support both Traditional MIPS and MVP submission
- Provision for extra submission-season support to providers
For Provider Orgs
- Verify that the chosen reporting path still reflects the intended strategy
- Confirm that reweighting decisions, measure selections, attestations, and documentation are complete
- Make sure the data being shared with Registry or CMS is complete and usable
- Ensure one person has the authority to drive the final submission process
What to review now→
Reweighting and hardship application decisions
Audit support and attestation documentation
Submission path and timeline
Data required for submission in the correct format
Final validation of Quality, PI, and IA category inputs before submission
Submission readiness checklist
| Checkpoint | EHR readiness | Provider Org readiness |
|---|---|---|
| Measure logic validated | Final logic has been tested and confirmed | Review logic and score assumptions with the EHR and Registry |
| Documentation complete | ONC Certification, required attestations, and audit readiness are in place | Confirm documentation for PI, IA is complete, or a plan is in place |
| Category rules aligned | Numerator, denominator, completeness, case minimums, and measure logic are verified | Review all measures, understand preliminary scores, and finalize the reporting plan |
| Submission path confirmed | File format, data aggregation, and submission workflow are ready | Confirm that all requirements for the selected submission path are complete |
Where MyMipsScore improves coordination
MyMipsScore brings measure logic, validation, documentation, and submission readiness into a single, structured process, so teams don't have to stitch together the final submission tasks under the pressure of deadlines.
Review your submission readiness →
Step 10. Understand the MIPS final score and its financial impact
The final step is not just about calculating the MIPS score. It is about providing both EHR and Provider Organization leadership with clarity on the financial impact of supporting MIPS efforts and performance. It also provides them with insight into the costs and benefits of timely readiness versus a pre-submission scramble.
The Challenge
Too many organizations reach the end of the MIPS journey without a clear view of their projected MIPS final score, what is driving it, and whether there is still room (and time) to improve it.
The impact on the organization
Leadership needs more than a MIPS score estimate. They need a clear view of the expected payment impact, the factors shaping the result, and whether the outcome reflects early planning or late-stage recovery. That visibility helps EHRs gauge the strength of their MIPS support, and helps Provider Organizations make better financial and operational decisions before submission closes.
For EHRs
- Maintain support for current measure logic, PI readiness, and specialty alignment
- Support specialty-relevant measures for both Traditional MIPS and MVPs
- Ensure measure calculations use current logic and are accurate
- Provision for extra support during the MIPS submission period for customers
For Provider Orgs
- Confirm reweighting and final category weights
- Understand expected score range
- Assess the payment adjustment implications of the score
- Review projected financial impact before submission closes
Payment Adjustment
The final MIPS score determines the Medicare Part B payment adjustment applied two years later. For the 2026 performance year, the maximum payment adjustment remains ±9 %.
A score of 75 (neutral) is required to avoid a penalty.
The negative payment adjustment is not a simple pass-fail outcome. CMS uses a scaled approach for scores below 75.
Scores between 0 and 18.75 will receive the maximum penalty.
For scores between 18.75 and 74.9, the penalty decreases as scores approach the neutral performance threshold.
Scores above 75 are eligible for a positive payment adjustment.
Since MIPS is a budget-neutral program, CMS uses the funds collected through penalties to make the positive payment adjustments.
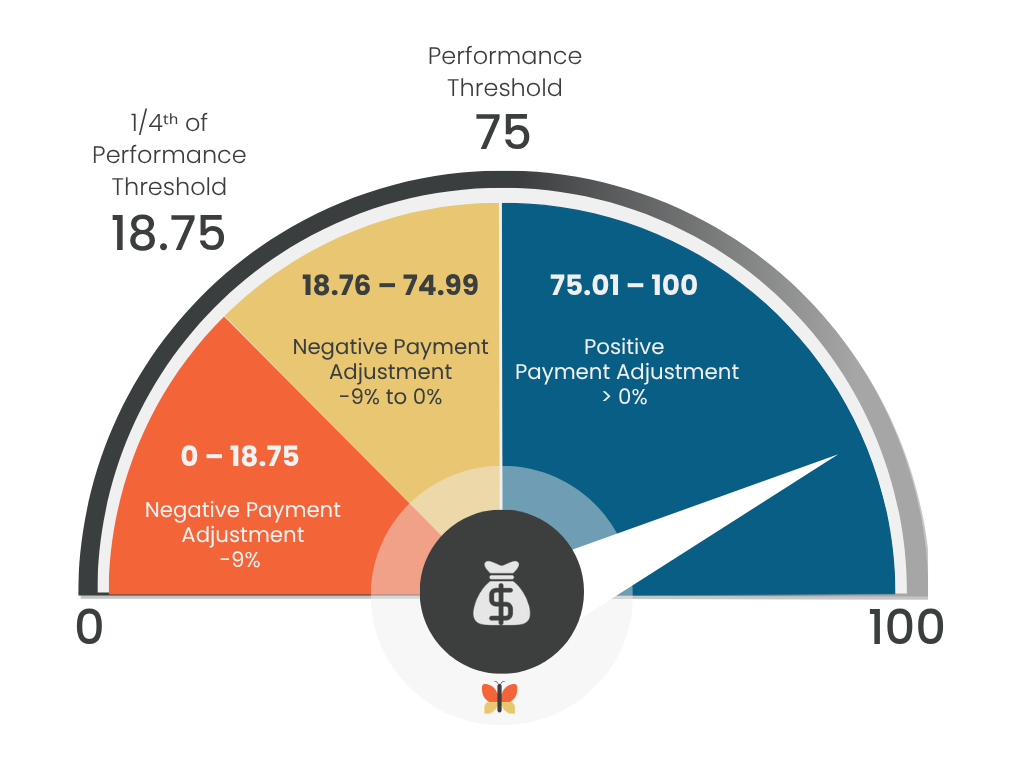
This graphic illustrates how MIPS performance scores translate into payment adjustments, showing the threshold for positive incentives and the ranges where providers may receive neutral or negative adjustments.
MyMipsScore simplifies the MIPS score and its financial impact
MyMipsScore gives EHRs and Provider Organizations early visibility into measure scores, category performance, and final MIPS score estimate based on various factors, so decision-makers are not forced to wait until the outcome is locked. They can evaluate various measures, submission options (individual or group), and reporting paths (Traditional MIPS, MVP, or MIPS APM) and make the decision that yields the best outcome for them.
Review 2026 MIPS financial impact →
Bring MIPS into one connected workflow
MIPS affects more than reporting. For EHRs, MIPS support is not just a compliance feature. It can improve customer experience, strengthen product stickiness, and create a new paid service line. For Provider Organizations, it affects readiness, operational coordination, and financial outcomes.
As a CMS-Qualified Registry and an ONC-certified health IT, MyMipsScore helps both sides manage the process more effectively by connecting current-year logic, score visibility, audit-ready documentation, and submission readiness. The result is a more integrated and manageable process for both EHRs and Provider Organizations.
For EHRs
Turn MIPS support into a customer and revenue advantage
MyMipsScore helps EHRs offer integrated MIPS support that is easier for customers to use and harder for competitors to match. Instead of sending providers elsewhere for help, EHRs can support them within the same relationship, improve customer satisfaction, strengthen retention, and create a separate source of revenue through paid MIPS support.
For Provider Orgs
Get a more connected and less stressful MIPS process
MyMipsScore helps Provider Organizations manage performance, documentation, and submission in a more structured way, with clearer score visibility and fewer last-minute surprises. That makes it easier to stay on track and easier for leadership to understand the likely payment adjustment impact before submission closes.
Discover a more integrated way to manage MIPS
A more integrated MIPS process creates value on both sides: stronger customer support for EHRs and a less stressful reporting experience for Provider Organizations, by making MIPS more manageable and less vulnerable to avoidable errors.